Sensitivity vs. Specificity in Disease Diagnosis
Sensitivity and specificity are two important statistical terms used in assessment of disease risk. Sensitivity refers to the ability of a test to accurately identify those with the disease, while specificity refers to the ability of a test to accurately identify those without the disease. The following formulas help calculate these quantities:
sensitivity = true positives / (true positives + false negatives)
Essentially, you are calculating what fraction of the truly positive cases are correctly identified as positives.
specificity = true negatives / (true negatives + false positives)
Essentially, you are calculating what fraction of the truly negative cases are correctly identified as negatives.
Let’s try a few USABO practice problems to understand this concept in context.
Problem 1 - USABO Semifinal Exam 2008

The exposition of the problem suggests that your friend is likely mistaken about the status of his condition. The 98% sensitivity indicates that 98% of true positive cases (which I am assuming is only testing for carriers, as disease phenotypes will be obvious) are identified as positive. The 90% specificity indicates that 90% of truly negative cases were indicated as negative.
positives - 98% identified as positive, 2% identified as negative
negatives - 90% identified as negative, 10% identified as positive
The question asks for the probability that he is part of the 10% bucket (“NOT a carrier”). To figure this out, we need to find the probability that any given individual is positive, and we will use this to weigh out our categories. Using Hardy-Weinberg equilibrium, we know:
if recessive allele = a, frequency of a = sqrt(1/10000) = 1/100 = 0.01
frequency of A = 1 - frequency of a = 1 - 0.01 = 0.99
P(positive result) = P(Aa) = 2 x 0.99 x 0.01 = 0.0198
Out of a population of 100000, 1980 individuals will thus be carriers. So there are 1980 positives and 100000 - 1980 = 98020 negatives in the population. I am unsure of if we should include the autosomal recessives in our count of negatives, as they technically do have the disease, but they are not carriers either. The question doesn’t specify, but I think either way, their contribution would be negligible. So let’s keep going.
10% of 98020
= 9802. 9802/(total population who got a positive result)
= 9802/(0.98 x (100000-98020) + 0.10 x 98020)
= 0.83 = E.
WOOOOOO BABYYYYY
Problem 2 - USABO Semifinal Exam 2014

If the test is sensitive but not specific, it means that positives are likely true, while negatives are likely false. That means the sensitivity is good, so it would likely not be affected by SNP tech error rates. And either way, an inherent error rate would affect both sensitivity and specificity. 105 is false. Lack of sensitivity means only positives need to be looked upon with suspicion; you don’t know how to feel about negatives. 106 is false. 107 and 108 fit the definition of sensitivity and specificity respectively, so they are true.
———
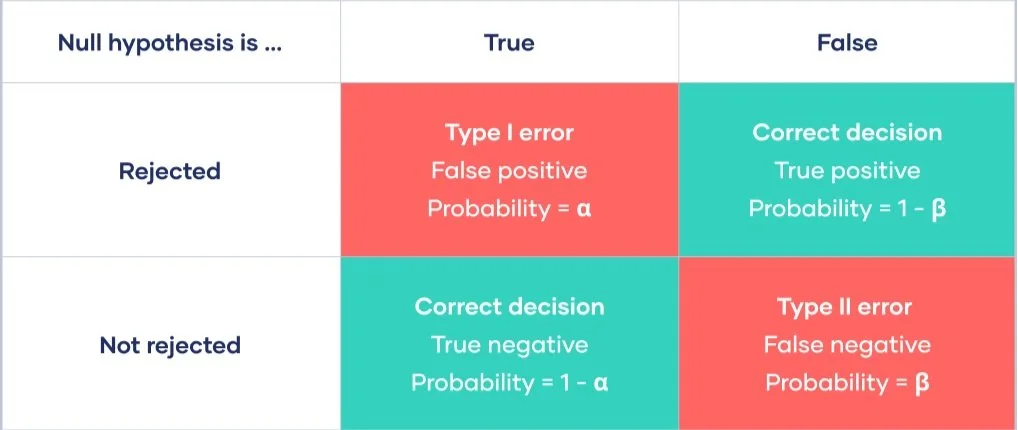
Okay. One more thing. Sensitivity and specificity are connected to another statistical concept: type I and type II errors. Increasing sensitivity decreases type II errors, while increasing specificity decreases type I errors.
I enjoyed writing this. Thanks for reading!